Pain in the hip: FAI/ femoroacetabular impingement and what to do about it
Hip pain? You’re not FAI-king it!
What is FAI?
First of all, let’s take a look at your hip and what exactly it is. The hip joint is a ball-and-socket joint. This means that it consists of one “ball” part (the head of your femur/thigh bone), and a “socket”, which is the deep recess (acetabulum) in your pelvis that allows the “ball” to sit in. Most of the time, this ball-and-socket joint moves smoothly through your full range of movement. However, in some situations, you may get pain due to various hip conditions.
In this blog post, we will be discussing a common condition named femoroacetabular impingement (FAI) syndrome. FAI syndrome is a symptomatic condition caused by abnormal contact between the femur and acetabulum, which can present as hip pain. FAI can present in three patterns: cam, pincer and mixed.
Cam morphology is the irregular formation of the femoral neck, which increases the area available for contact with the “socket” of the hip joint.
Pincer morphology occurs where there is overcoverage of the “socket” over the “ball”. Some hips may present with a combination of both cam and pincer morphologies, and are termed as a mixed pattern.

Source: https://orthoinfo.aaos.org/en/diseases--conditions/femoroacetabular-impingement/
How is it diagnosed?
In order for FAI syndrome to be diagnosed, there has to be a combination of symptoms, objective assessment findings and radiological findings. Some people may have incidental findings on a scan of their hips without experiencing pain or symptoms, and this would not be diagnosed as FAI syndrome.
What are the symptoms?
The clinical presentation of FAI is usually hip pain, which may be accompanied by clicking, catching, locking, giving way or stiffness (Griffin et al, 2016). In combination with a detailed subjective interview, practitioners may perform a few tests, such as the FADIR test which involves moving the hip into certain positions to elicit symptoms.
Pain from FAI syndrome is diverse in its location, nature and severity. Most patients report pain in the groin and/or hip, but pain can also be located in the lateral hip, glute, knee, lower back, or in various parts of the thigh (Griffin et al, 2016).
Reproduction of pain is usually movement related or due to sustained postures. This can look like symptoms during or after high intensity activity, or pain with movement going through a larger than normal range of motion (such as dance and gymnastics), or symptoms due to prolonged or sustained positions such as sitting for long periods of time.
Patients with FAI often have pain especially at the end of their available range of motion. For example, sitting in deep chairs, or high kicking. These types of activities bring the hip joint into the end of its available range, where the impingement occurs, thus leading to symptoms.


High kicks (Left) bring the hip into its end-range position. Soccer players or dancers may do this repetitively during training. Deep or low seats cause more hip flexion in sitting (right), which can cause irritation in the hip joint if prolonged.
How is it managed?
The common approaches to managing FAI are conservative interventions such as various types of injections and physiotherapy management or more invasive interventions such as surgery (hip arthroscopy).
The symptomatic hip often has reduced strength in hip and core musculature, particularly in hip adduction and flexion (Diamond et al, 2015). However, this varies with the individual, with some studies showing that male and females have strength deficits in different muscle groups (Freke et al, 2018). Thus, each patient should be carefully assessed to identify specific deficits, and provided a tailored strengthening program of these muscles to reduce symptoms and maintain joint health in the long term. Additionally, aggressive and painful stretching into the end of available range is not recommended as this may put the hip joint in positions that expose the cartilage to damage (Wall et al, 2016).
Studies have also shown that people with FAI also tend to have altered control of hip and pelvis movement when compared to populations without FAI syndrome (Lewis et al. 2018; Bagwell and Powers, 2019). This may present as a reduced ability to tilt the pelvis backwards in movement. Hence, neuromuscular control with unilateral exercises such as step ups with a focus on reduced trunk and hip flexion and more posterior pelvic tilt could be included to re-train movement of the joint in a less aggravating position.

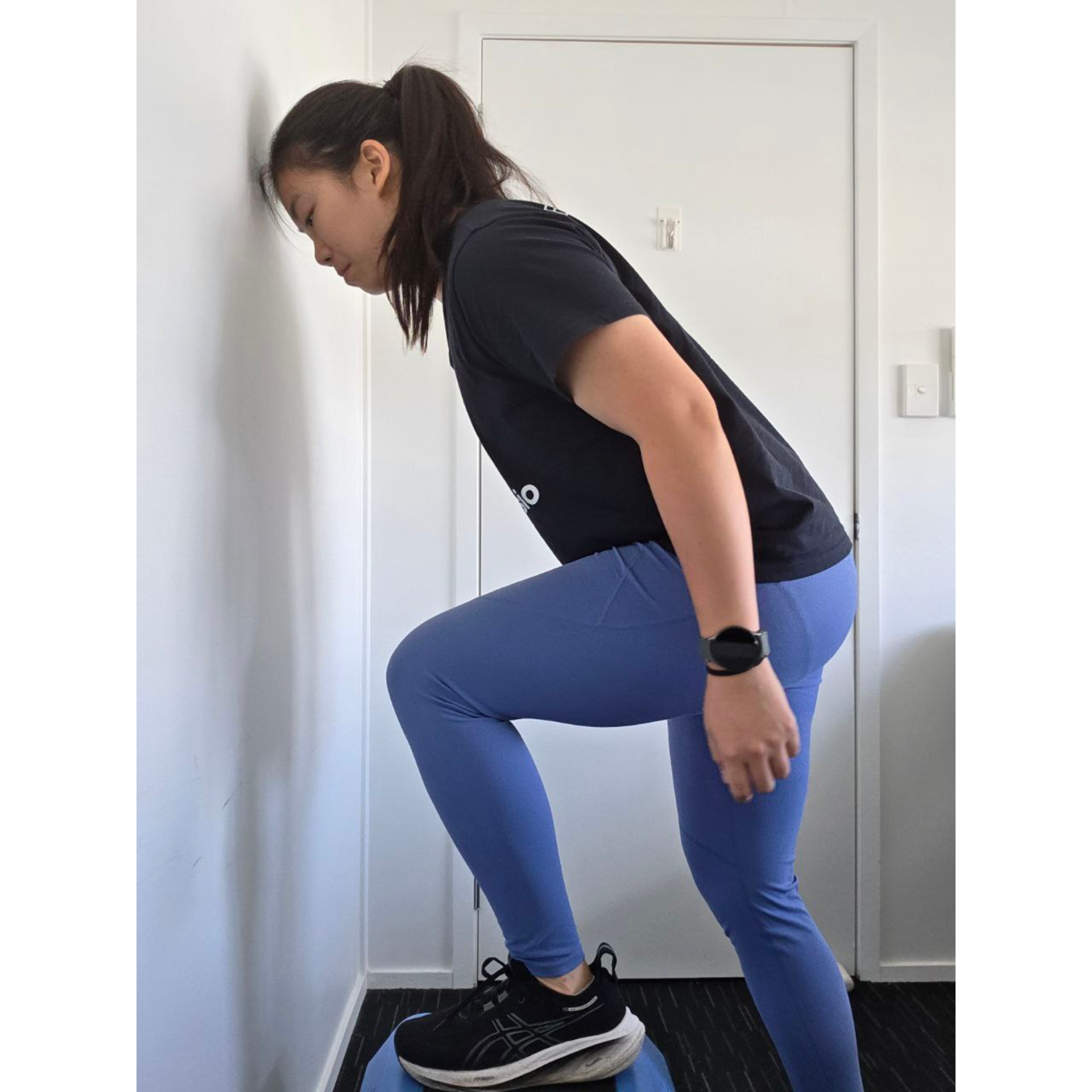
Comparison of step up technique. Left: Step up with less trunk flexion which may be less irritable for FAI. Right: Step up with more hip and trunk flexion which may increase irritation of FAI.
Other than building strength in the symptomatic hip to reduce deficits for better long term outcomes, it is also important to have strategies for short-term relief. Individuals with FAI can be recommended non-steroidal anti-inflammatories to reduce acute inflammation and pain. As an adjunct to pain relief, patients can also be taught activity and lifestyle modification to reduce irritation of the hip and reduce aggravating activities. For example, people with FAI can be encouraged to lean backward when sitting for prolonged periods. This is so that the hip is not in sustained hip flexion, which is an aggravating factor.
The same principle can be applied to exercise prescription where individuals can be recommended to avoid end of range positions in squats and leg press, or to alter leg positioning to reduce impingement positions.




- Narrow squat with feet and knees parallel which may be less comfortable due contact in hip joint vs 2. wide stance squat with feet and knees pointed outwards which may be more comfortable. 3. End of range deep squat which may be aggravating vs 4. shallow squat (right) which may be more tolerable.
In certain situations, physiotherapy alone may not be sufficient to reduce symptoms. In these cases, injections may be a suitable adjunct to physiotherapy treatment. Injections available for treatment of FAI syndrome include corticosteroid, hyaluronic acid, platelet rich plasma (PRP), or bone marrow aspirate concentrate (BMAC) injections. Of these injections, studies have shown that hyaluronic acid and corticosteroid injections (CSI) demonstrate short-term benefit. However, CSI is associated with possibly poorer long term outcomes of the joint cartilage and hence should be used cautiously, and in conjunction with exercise (Dancy et al, 2025). PRP and BMAC injections have not had high quality evidence to support their use and thus further research is required (Dancy et al, 2025).
In some individuals, physiotherapy and injections may not be able to sufficiently reduce symptoms, or they may have significant changes in joint range or radiological findings. For these individuals, surgery is another option to reduce risk of progression of hip osteoarthritis (OA) (Dancy et al, 2025). This is particularly pertinent in hips with large cam-type lesions, as the repetitive contact of the hip joint applies shear forces to the tissues in the hip joint which are proposed to cause changes to the labrum and cartilage and contribute to hip OA. Some studies have shown that surgery such as arthroscopy may reduce the risk of progression of OA by reshaping the ball-and-socket joint to reduce the premature and abnormal contact. However, given the cost involved and other potential side effects of invasive management, surgery may be reserved for situations where conservative treatment yields no benefits and progression of symptoms is occurring, or for high risk populations described above.
So what should I do if I think I have FAI?
If the symptoms of FAI sound similar to what you are experiencing, the good news is you can start implementing some of the tips as discussed above:
- Reducing time in aggravating positions such as sitting in a deep seat
- Temporarily avoiding moving/stretching into end range and painful positions such as deep squats or high kicks
- Adding hip and core strengthening exercises with a focus on the painful side to build strength
Our physiotherapists are also experienced in assessing specific strength deficits and identifying if your movement patterns may be aggravating your symptoms. As such, if you are experiencing symptoms that are not improving with self-management, it can be worth booking an appointment with one of our physiotherapists who can help you identify specific areas to target and give specific advice tailored to your situation.
Click here to start your hip rehabilitation with one of our team
References:
Bagwell, J. J., & Powers, C. M. (2019). Persons with femoroacetabular impingement syndrome exhibit altered pelvifemoral coordination during weightbearing and non-weightbearing tasks. Clinical Biomechanics, 65, 51-56.
Dancy ME, Oladipo V, Boadi P, Mercurio A, Alexander AS, Hevesi M, Krych AJ, Okoroha KR. Femoroacetabular Impingement: Critical Analysis Review of Current Nonoperative Treatments. JBJS Rev. 2025 Apr 16;13(4):e24.00211. doi: 10.2106/JBJS.RVW.24.00211. PMID: 40238927; PMCID: PMC11939100. https://pmc.ncbi.nlm.nih.gov/articles/PMC11939100/
Diamond LE, Dobson FL, Bennell KL, et al. Physical impairments and activity limitations in people with femoroacetabular impingement: a systematic review. British Journal of Sports Medicine 2015;49:230-242.
Freke M, Kemp JL, Svege I, et alPhysical impairments in symptomatic femoroacetabular impingement: a systematic review of the evidence. British Journal of Sports Medicine 2016;50:1180
Griffin DR, Dickenson EJ, O'Donnell J, et al. The Warwick Agreement on femoroacetabular impingement syndrome (FAI syndrome): an international consensus statement. British Journal of Sports Medicine 2016;50:1169-1176.
Lewis, C. L., Loverro, K. L., & Khuu, A. (2018). Kinematic Differences During Single-Leg Step-Down Between Individuals With Femoroacetabular Impingement Syndrome and Individuals Without Hip Pain. The Journal of orthopaedic and sports physical therapy, 48(4), 270–279. https://doi.org/10.2519/jospt.2018.7794
Terrell, S. L., Olson, G. E., & Lynch, J. (2021). Therapeutic Exercise Approaches to Nonoperative and Postoperative Management of Femoroacetabular Impingement Syndrome. Journal of athletic training, 56(1), 31–45. https://doi.org/10.4085/1062-6050-0488.19
Wall, P. D., Dickenson, E. J., Robinson, D., Hughes, I., Realpe, A., Hobson, R., Griffin, D. R., & Foster, N. E. (2016). Personalised Hip Therapy: development of a non-operative protocol to treat femoroacetabular impingement syndrome in the FASHIoN randomised controlled trial. British journal of sports medicine, 50(19), 1217–1223. https://doi.org/10.1136/bjsports-2016-096368